Examination of the hip video
Watch now
A short video demonstrating how to examine the hip joint.
Look
- With the patient standing, assess for muscle wasting (gluteal muscle bulk in particular).
- With the patient lying flat and face up, observe the legs, comparing one side with the other – is there an obvious flexion deformity of the hip suggesting osteoarthritis?
- If there is a suggestion of leg length disparity, assess true leg lengths using a tape measure. Measurements are taken from the anterior superior iliac crest to the medial malleolus of the ankle on the same side. Compare the measurements. In a fractured neck of femur, the leg is shortened and externally rotated. There may also be an indication of this on the patient’s footwear with excessive wear on one heel.
- Check for scars overlying the hip.
Feel
- Palpate over the greater trochanter for tenderness (suggestive of trochanteric bursitis) and in the groin for true hip joint problems.
Move
- With the knee flexed at 90°, assess full hip flexion, comparing one side with the other and watching the patient’s face for signs of pain.
- Assess for a fixed flexion deformity of the hip by performing the Thomas test. Keep one hand under the patient’s back to ensure that normal lumbar lordosis is removed. Fully flex one hip and observe the opposite leg (see image below). If it lifts off the couch, then there is a fixed flexion deformity in that hip. (As the pelvis is forced to tilt a normal hip would extend allowing the leg to remain on the couch.)

- With the hip and knee flexed at 90°, assess internal and external rotation of both hips. This is often limited in hip disease and internal rotation is frequently the first movement affected (see GALS screen).
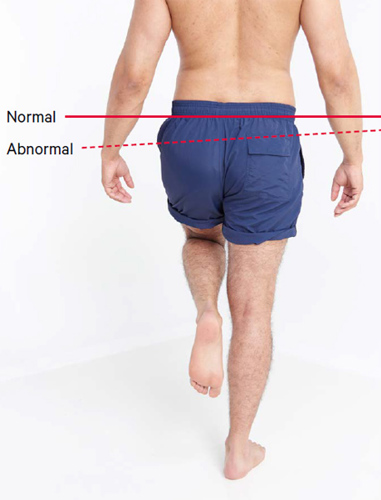
- Assess the hip and proximal (gluteal) muscle strength by performing the Trendelenburg test. This involves the patient alternately standing on each leg alone. In a negative test, the pelvis remains level or even rises. In an abnormal test, the pelvis will dip on the contralateral side (see image below).
Function
- Ask the patient to walk – look for an antalgic or Trendelenburg gait. An antalgic gait simply means a painful gait, normally resulting in a limp. A Trendelenburg gait results from proximal muscle weakness and commonly results in a ‘waddling’ walk.