How does the shoulder work?
Your shoulders each have two joints, making them the most flexible parts of your body.
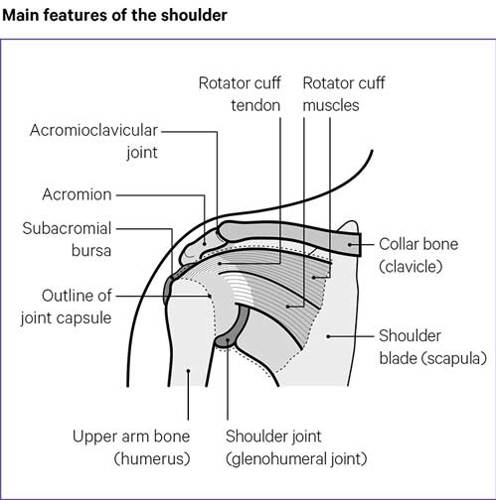
The main shoulder joint – the glenohumeral – is a ball-and-socket joint. It’s called this because the top of the upper arm bone – the humerus – is shaped like a ball. This ball fits into the shoulder blade bone, which acts as the socket, giving your shoulder a wide range of movement.
But, the shoulder socket is very small, compared to other ball-and-socket joints, such as the hip. It’s held together and controlled by a covering of muscles, which are secured to the bones by strong cords called tendons.
These muscles and tendons form a capsule around the joint and support its movements, but can make it more likely to dislocate than other joints.
Inside the capsule is the synovium, which produces fluid that lubricates the joint and keeps the cartilage healthy. The cartilage helps protect your bones from any impact and sits between the bones of your shoulder joints to stop them rubbing together.
Above the main shoulder joint there’s a smaller joint where the top of the shoulder blade – the acromion – meets the collar bone.
This is known as the acromioclavicular joint. It helps the larger joint below to move through its full range, particularly when you’re raising your arm, lifting or throwing.
Causes
Most shoulder problems only affect a small area and should last a relatively short time.
But sometimes the problem in your shoulder could be part of a wider, long-term condition such as, osteoarthritis or polymyalgia rheumatica.
It’s fairly common for people with rheumatoid arthritis to have pain and swelling in their shoulders.
Osteoarthritis is less likely to affect your shoulders than other joints, unless you’ve injured them in the past.
There are several other possible causes of shoulder pain, such as:
- inflammation, where your shoulder becomes hot, red, swollen and painful as a natural reaction to an infection or injury
- damage to the muscles and tendons around the shoulder
- tension in the muscles between the neck and shoulder – this is usually down to your posture in your upper back or neck, and is often linked the way you stand or sit when you’re using a computer or at work
- inflammation in the bursa – a fluid-filled cushion which normally helps the muscles and tendons slide smoothly over the shoulder bones
- damage to the bones and cartilage, which can be caused by arthritis.
It’s also possible the pain you’re feeling in your shoulder is coming from a problem in another part of your body, such as your neck.
Problems in your neck can make your shoulder blade or upper outer arm painful. When this happens it’s known as referred pain or radiated pain. If you’re feeling a tingling sensation in your hand or arm, as well as pain in your shoulder, it’s likely to be from a problem in your neck.
When to see a doctor
Unless you’ve had a serious injury or get a sudden, continuous pain, you can usually treat your shoulder pain without having to see your doctor.
If, after two weeks of treating yourself, you feel the pain isn’t any better you should see your doctor or a physiotherapist.
You should also see your doctor as soon as possible if you:
- develop severe pain in both shoulders
- also have pain in your thighs
- feel feverish or unwell.
These can be signs of the condition called polymyalgia rheumatica, which needs prompt treatment.
Managing symptoms
There are several ways you can help your shoulder pain:
Painkillers
Simple painkillers, such as paracetamol, or non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen tablets and gels, from a chemist or supermarket can help.
A pharmacist should be able to give you good advice on what could work best for your condition. But don’t use them for more than two weeks without seeking further medical advice.
Heat or cold therapy
An ice pack may be helpful if your shoulder is painful after a minor injury or if it’s swollen and warmer to touch than the other side.
You can use a bag of frozen peas, wrapped in a damp towel to protect your skin. Leave it in place for no longer than 20 minutes.
Alternatively, heat packs can help with most other types of shoulder pain, particularly if your muscles feel sore and tense.
Chemists and sports shops sell reusable heat pads. Or you could use a microwaveable wheat bag or a hot-water bottle, wrapped in something dry, such as a towel, on the painful area for up to 20 minutes.
Posture
Bad posture or working habits, such as slouching at your desk, can make your shoulder problems worse.
Try these tips:
- When you’re sitting down try to avoid leaning forwards and resting on your arms too much.
- Try to relax your shoulders and let your arms hang by your sides, rather than gripping them tightly into your sides, especially if some of the pain is coming from your neck.
- Change your position often.
- Sit in an upright position.
- Support your lower back with a pillow, cushion or a chair with lumbar support to improve your upper body posture.
- If your arm is really sore, keep it supported and comfortable with a cushion or pillow on your lap.
- Use a mirror to practise holding your shoulder blades down and back – focus on your shoulder blades and imagine keeping your chest still and pulling the blades downwards and back towards each other.
If your shoulder is painful when you lie down, try:
- lying on your good side with a pillow under your neck
- using a folded pillow to support your painful arm in front of your body
- placing another pillow behind your back to stop yourself rolling onto your painful side
- using one or two pillows under your painful arm for support, if you prefer to sleep on your back.
Reduce the strain
Generally, it’s best to carry on with your normal activities as much as you can – but don’t overdo it. You may need to pace yourself more than usual and try to gradually do a bit more each day.
There are ways you can do some tasks slightly differently, so you don’t hurt your shoulder.
At home:
- When vacuuming, keep your upper body upright with the vacuum close to your body, and use short sweeping movements.
- Only iron essential items, and make sure the ironing board is at waist height.
- Use a trolley or a backpack to carry shopping. Or you could divide the weight between two bags and carry one in each hand. Alternatively, use bags with long straps and carry them with the straps crossed over your body from shoulder to hip. The key is to try to spread the load of what you want to carry.
- Ask your friends with cars if they could help you out by adding anything heavy to their shopping list.
- Use a delivery service for heavy or bulky shopping.
- Limit the amount of time you spend sitting looking down at tablets and mobile phones. Instead use a stand on a table to reduce neck strain.
- If you have to do tasks that involve raising your arms or sweeping movements, give yourself plenty of time and ask someone to help you. Take lots of breaks and try to switch tasks and positions
At work:
- Try to maintain a good posture when you’re sitting or standing. Avoid holding your neck in fixed or twisted positions.
- If you sit or stand at a workstation, such as a desk or workbench, try to get up and move around every so often. Try to gently move your shoulders and neck through their full range of movement regularly, to stop them getting stiff and sore.
- If you use a computer keep the keyboard and monitor directly in front of you, so you don’t have to turn your head or twist your body. Keep the mouse within easy reach so you don’t have to stretch for it.
- A good chair that supports you properly and can be adjusted to your needs could also help you keep a good working position. An occupational health advisor or your manager could be able to help you with this.
- When using the phone, don’t hold the receiver to your head with your shoulder. If you’re on the phone a lot, use a telephone headset.
- Avoid any manual work that hurts while you’re doing it.
Your line manager or human resources department should be able to help you. Some companies have an occupational health department that might be able to give you some advice and support.
You could also contact your local Jobcentre Plus office, who can put you in touch with advisors specialising in physical difficulties at work. Take a look at our information on working with arthritis and joint pain.
If you’ve been diagnosed with a condition your employer is legally required to make reasonable adjustments to your work and your working environment to help you do your job. Amongst other changes, they have to help you adapt your workstation, perhaps by changing your chair, the equipment you use or how it is laid out so that you can still do your job.
Gov.uk has advice on what reasonable adjustments your employer is expected to make.
Rest and exercise
It’s important to keep active, even if you don’t feel you can do much. If you try to get a good balance between rest and activity it should help stop your shoulder getting stiff. Here are some exercises for the shoulders that might help.
Try avoiding movements that really hurt. Raising your arm above your shoulder or holding it away from your body can be very painful so it’s best to try to avoid movements like this as much as possible until it becomes less painful.
If you have to raise your arm you can reduce the strain on your shoulder by:
- keeping your elbow bent and at the side of your body
- keeping your palm facing the ceiling when reaching up.
To lower your arm, bend your elbow, bringing your hand closer to your body.
You may find it more comfortable to do exercise after putting ice on your shoulder or taking painkillers. Remember to wrap ice in a damp towel, so you don’t burn or irritate your skin.
Complementary treatments
There are several complementary treatments that some people find relieve their shoulder pain. Some are available on the NHS, such as acupuncture. But, on the whole the NHS doesn’t recommend complementary treatments, as there’s no good evidence that they work.
Complementary treatments are relatively safe. But, you should always talk to your doctor before you start using them in case they interfere with specific treatments you’re already taking.
Before starting any therapy or treatment, it’s important to make sure the therapist or supplier has a set ethical code, is legally registered and fully insured. We have more information about the organisations that oversee complimentary treatment practitioners and what you should expect from complementary and alternative therapists.
Because you will, more than likely, be paying for any complementary treatments, you should consider whether or not they’re helping your condition before deciding if you’re going to keep using them.
We have information on complementary treatments, including acupuncture, aromatherapy, manipulative therapies – such as chiropractic or osteopathy treatments, supplements, and much more.
Related information
-
Let's Move with Leon
Sign up to Let’s Move with Leon our weekly email programme of 30-minute movement sessions, presented by fitness expert Leon Wormley.
-
Let's Move
Sign up to Let’s Move to receive a wide range of content about moving with arthritis – from exercise videos to stories and interviews with experts – straight to your email inbox.
Diagnosis
Each shoulder problem has its own pattern of symptoms that can help your doctor or a physiotherapist make a diagnosis. Most conditions make it painful to use or move your shoulder, but some make your shoulder feel stiff.
Your doctor or physiotherapist will need to see which movements are the most painful, as this could show where the problem is. They will usually ask how the problem started, how it has developed and how it affects your daily activities.
If you can, try to write a few notes about when and how the problem started and what makes it feel worse before your appointment. This will help you get a more accurate diagnosis.
Usually your physiotherapist or doctor can recommend the best course of treatment once they’ve diagnosed what your condition is. However, they may send you for further tests if they suspect your problems are being caused by arthritis or a more complicated condition.
What tests are there?
Blood tests aren’t usually needed for most shoulder problems, but they’re sometimes used to rule out other conditions, including some types of arthritis.
X-rays are good for looking for problems with the bones in your shoulder and minor changes in the joints. However, small changes are quite common and may not be the cause of your trouble.
X-rays can only show bones and other hard substances, but they won’t show injuries to soft tissue like muscles.
An ultrasound scan can show swelling, as well as damage and problems with the tendons, muscles or other soft tissues in the shoulder. It uses high-frequency sound waves to examine and build pictures of the inside of the body.
You may be referred for magnetic resonance imaging (MRI) scans if your doctor suspects a more complex problem with the soft tissue in your shoulder. An MRI uses radio waves to build a picture to show what’s happening to the bones and soft tissue, such as the muscles and tendons, inside your shoulder.
Sometimes dye is injected into the shoulder before the MRI to get a clearer picture – especially in cases of shoulder dislocation.
Nerve conduction studies can show whether your problems are being caused by the nerves in your arm being pinched or irritated.
They measure the electrical activity in the muscles and nerves. It’s common to feel slight pain or discomfort, like a tapping on the skin, but the test doesn’t last long.
Specific shoulder conditions
Some of the specific conditions that affect the shoulder include:
Calcific tendonitis and calcific periarthritis
Sometimes pain, swelling and difficulty moving your shoulder is caused by calcium crystals that form inside a tendon. Tendons are the strong cords that attach muscles to bones.
We all need the mineral calcium in the body, as it helps make bones and teeth strong. But sometimes, if you have too much of it in the body, sharp, tiny, crystals can form in the wrong places.
If they form in tendons, this is called calcific tendonitis.
This can happen at various places around the body, including the shoulder.
Calcium crystals can then shed from a tendon and cause pain and swelling around a joint. This is called calcific periarthritis.
Steroid injections often work well to reduce swelling. But sometimes the calcium deposits may need to be removed by keyhole surgery.
Frozen shoulder (adhesive capsulitis)
If you have a frozen shoulder the capsule around the joint has become too tight, stopping you moving your shoulder. We don’t always know why this happens, though sometimes it follows an injury, a heart attack or stroke, and it’s more common in people with diabetes who can’t produce insulin properly.
The condition will usually resolve itself in time, but it may take as long as two to three years.
The pain can be severe and you may feel sudden muscle pains, called muscle spasms, especially at night. You may need painkillers to help.
Sometimes a treatment called a volume hydrodilatation is used for frozen shoulder. This involves a combination of:
- a steroid injection, guided into the painful area by ultrasound
- local anaesthetic to numb the area
- a solution of salt and water.
This treatment is injected into the shoulder to stretch the lining of the capsule. It can be a bit painful, but your shoulder should feel less painful afterwards. Most people find it very helpful, but for some people it will only work for a short time.
Physiotherapy or a steroid injection on its own may also help.
Most people with frozen shoulder make a full recovery. But, if your problem continues even after trying other treatment options, you may need to consider surgery.
Your doctor or physiotherapist will talk to you about which operation will help your condition most – keyhole techniques to release the tight capsule around the joint or surgery to manipulate the joint.
To stop the problem returning you’ll need to follow a programme of exercises afterwards. It’s important to do your exercises regularly to get your shoulder back to full use and keep it working properly.
Osteoarthritis
Osteoarthritis is a common condition which can affect any joint. But it’s less common in the shoulder, unless you’ve had a previous injury, or your shoulder joints have been put under extra stress.
In osteoarthritis of the shoulder the cartilage becomes thinner and tiny bits of extra bone, called osteophytes, can form on the joint and change its shape.
This can be very painful and makes moving your arm and shoulder difficult. It might be painful reaching across your body, reaching up above your head or when you lie on the affected side.
Your treatment will depend on the level of pain you’re in and how it has affected your range of movement. Physiotherapy can help but you may also need painkillers. If you have a flare-up, where your condition suddenly becomes worse, you might need a course of non-steroidal anti-inflammatory drugs (NSAIDs).
A steroid injection may be helpful.
If non-surgical treatments don’t help and your osteoarthritis is really affecting your quality of life, you may need to talk to your doctor and physiotherapist about the pros and cons of joint replacement surgery. See our information on Shoulder and elbow replacement.
Polymyalgia rheumatica
Polymyalgia rheumatica typically causes pain and stiffness in the muscles of your shoulders and pelvis. It develops quite quickly over a week or so and is especially bad in the mornings.
If you have pain in both shoulders and in your hips, and you’re feverish or feel generally unwell, try to speak to your doctor as soon as possible. The earlier polymyalgia rheumatica can be treated the better, as it can cause other complications, such as inflammation of the blood vessels in the head.
It responds well to treatment with steroid tablets, though the treatment may need to be continued for a year or more.
Referred neck pain
If you’ve been told the pain in your shoulder is caused by referred pain it could be coming from an injury or inflammation in your neck.
Often, it’s linked to the sensation of pins and needles in your arm or hand, as well as pain that travels down your arm. It can also be known as radiated pain.
Occasionally, you may be sent to a neurosurgeon, but sometimes the condition is only confirmed when physiotherapy treatment to the neck resolves the problem.
Lung conditions
Conditions affecting the lungs, for example cancer, can sometimes cause pain in your shoulder. Cancer is more of a risk if you’re a smoker and over 40.
If you’ve been experiencing unexplained pain for more than three weeks your doctor may recommend you have a chest x-ray. You should also tell your GP if you’ve had any unexplained weight loss or night-time sweating.
Rheumatoid arthritis
Rheumatoid arthritis is a type of inflammatory arthritis which typically starts in the hands and feet, but can affect the shoulders.
The inflammation affects the lining of the joint capsule, known as the synovium but may, after a period of time, cause damage to the cartilage, bones and ligaments.
There’s currently no cure, but there are many different treatments available. Some of these will help ease the symptoms, while others can slow down or halt its progression.
Joint replacement surgery can help if the joint is badly damaged by the arthritis.
Tendon problems
Various tendons in and around your shoulder can become inflamed, damaged or sore. These can cause a range of different problems.
Shoulder impingement or painful arc syndrome
The rotator cuff is a group of muscles and tendons that keep the upper arm bone held in the shoulder blade socket.
Pain from a problem with the rotator cuff is often called shoulder impingement. The condition causes swelling, pain or damage to the tendons of the rotator cuff. This can make it painful and difficult to move your arm properly.
You may find it painful and difficult to lift your arm away from your body, particularly if you’re trying to lift your arm above your head. Your arm may feel weak or you may have a dull lingering pain in your upper arm.
Really, it’s nothing to do with your tendons being trapped by bones, as was previously thought. Instead, it’s caused by overuse or age-related problems with the tendons themselves – but the name is still used. This condition can also be called painful arc syndrome.
Rest and physiotherapy are the main courses of treatment for a shoulder impingement. Your doctor may recommend an injection of steroids and a local anaesthetic, to help with the pain.
If the pain doesn’t settle, or comes back within a few months of treatment, you may need keyhole surgery.
Subacromial bursitis
Subacromial bursitis causes pain and swelling in the shoulder. It can make it difficult to raise your arm above your head.
It’s diagnosed when the subacromial bursa becomes inflamed. A bursa is a pocket of fluid that cushions a joint and allows bones to move freely. The subacromial bursa is the name for one particular bursa in each shoulder.
This condition is often caused by overuse or can be due to an injury from something like a fall. It can be linked to shoulder impingement.
Treatment will probably include rest, physiotherapy and NSAID tablets or creams. Surgery is rarely needed but could be recommended if your condition doesn’t improve.
Rotator cuff tear
A torn rotator cuff is more common in people over 40. Many people don’t remember hurting themselves beforehand. Some people have pain for a few weeks before they notice any difficulty moving their shoulder – though it isn’t always painful.
If you’ve torn your rotator cuff you may find it painful and difficult to raise your arm properly, especially above shoulder height.
Sometimes your neck and shoulder muscles over-compensate for this lack of movement, which can make you hunch your shoulders and can lead to neck pain.
The symptoms are similar to shoulder impingement and tendon tears are often only found after an ultrasound or MRI scan.
Physiotherapy is usually helpful, but some people need to have the torn part of their rotator cuff repaired by surgery.
Biceps tendonitis
The biceps tendon is connected to the biceps muscle on the front of the forearm and runs through the front part of the shoulder joint.
If this tendon becomes inflamed, you’ll find it painful to flex your elbow or bring your arm forwards. The front of your shoulder may also be sore. This is called biceps tendonitis.
Avoiding lifting your arm overhead will help it recover. You can help the pain by:
- using NSAIDs
- putting ice packs on the affected area
- doing gentle stretching exercises.
If your condition doesn’t improve your GP may recommend a local anaesthetic and steroid injection, to ease your pain.
Occasionally the tendon can rupture, causing bruising just above your elbow. This doesn’t stop you moving your shoulder or arm, but the biceps muscle may bunch. This can look unusual but it’s unlikely you’ll need surgery to repair the injury.
Treatment
If your shoulder pain doesn’t improve with simple home treatments, there are other alternatives your doctor can recommend for you to try:
Physiotherapy
Most shoulder problems will benefit from physiotherapy.
Physiotherapists are specialists who can help reduce your shoulder pain and show you how to improve the way your shoulder works by using a variety of strengthening and stretching exercise, massage and other therapeutic techniques.
They’ll work with you to improve your symptoms and help get your shoulder moving properly again. What they suggest for you will depend on whether your problem is short-term or a long-standing condition. Almost everyone will benefit from physiotherapy, using methods such as:
- exercises to strengthen weakened muscles, change their co-ordination and improve function
- advice on improving shoulder, neck and spine posture
- exercises to ease or prevent stiffness
- exercise to increase the range of joint movement
- applying adhesive tape to the skin to reduce the strain on the tissues, and to help increase your awareness of the position of the shoulder and shoulder blade
- manual treatments to the soft tissues and joints – such as massage and manipulation.
Your doctor can refer you to a physiotherapist, and in some areas you can refer yourself, but this referral could take a while.
You could see one quicker if you go privately but you would have to pay for this. You can find information about private physiotherapists in your area on the Chartered Society of Physiotherapy website.
Occupational therapy
If your shoulder problem is making daily activities difficult, such as dressing, washing and driving, it may help to see an occupational therapist.
An occupational therapist is a specialist trained to help you regain your independence by showing you how to change the way you do things. They can also advise you on how equipment or adaptations could reduce the strain on your shoulder at home, work, or while you’re driving.
They’ll be able to give you advice on how to change your movements to help prevent pain continuing or returning. If your place of work has an occupational health department, they may also be able to help.
You can also see an occupational therapist privately. You’ll be able to get an appointment quicker, but it will cost you money.
You can find a private occupational therapist in your area on the Royal College of Occupational Therapists website.
If you’re having problems at work, speak to an occupational therapist or the occupational health team if there’s one at your workplace. Otherwise, contact a Jobcentre Plus office to ask for advice. You can also find out more by looking at our pages on working with arthritis and joint pain.
Your doctor or physiotherapist can refer to you to see an occupational therapist, but you can also see an occupational therapist privately. You will be able to get an appointment quicker, but it will cost you money.
Find an occupational therapist that works privately on the Royal College of Occupational Therapists website.
Steroid injections
Steroid injections into the joint can ease some shoulder problems. The steroid is usually given with a local anaesthetic to ease the pain. You should find your shoulder pain improves quite quickly.
The injection reduces inflammation and allows you to move your shoulder more comfortably. The pain relief should also make your physiotherapy exercises easier, but you shouldn’t use your shoulder for anything too strenuous for the first two days after an injection.
It isn’t usually recommended to have more than two or three injections into your shoulder as this can do more damage to the joint. If the problem keeps coming back, your doctor will probably suggest further investigations to find a solution to the problem.
Sometimes the pain may be worse for a short time after the injection, but this doesn’t mean it’s gone wrong. You only need to seek advice if the pain continues for more than a day or so after the injection.
Some steroid injections may be done with the help of ultrasound imaging. This allows the inflamed tissues to be seen on a monitor and makes sure the injection is given in the correct area.
Surgery
Most shoulder problems improve without surgery. If you do need an operation it can often be performed using keyhole techniques, which require a smaller incision and tend to reduce your recovery time.
Keyhole surgeries include:
- subacromial decompression (see Figure 2) which involves trimming bone and tissue at the top of the shoulder. This can help if you keep having shoulder impingement which has not improved after physiotherapy and injections. It can give the rotator cuff tendons space to move freely
- repairing tears in the rotator cuff
- releasing the tight capsule of a frozen shoulder.
Conventional open surgery, where a surgeon makes an incision large enough to see the entire damaged area, may sometimes be needed. For example, to repair larger tears in the rotator cuff or for joint replacements.
Shoulder replacement is well established and can be very successful, particularly for osteoarthritis and rheumatoid arthritis, when severe pain stops you moving your shoulder properly.
There is also a newer type of shoulder operation called a reverse shoulder replacement. In this procedure the ball and socket are reversed. This helps if your rotator cuff tendons have been damaged by arthritis.
Physiotherapy and exercise are important after surgery to help restore movement – so be sure to do any recommended daily exercises.
You may not regain your full range of movement or strength after a total shoulder replacement, but it should be much better than it was after your shoulder problem started. Try to use your affected arm and shoulder carefully but confidently to help build and retain the muscle strength.
Research and new developments
We’re currently funding research aimed at improving the treatment of shoulder pain.
Our research has recently shown that subacromial decompression surgery, a common treatment for chronic shoulder pain, may have limited benefits and so should only be considered for people with this condition if other treatments haven’t helped. Our information on how decompression surgery may not benefit people with shoulder pain can tell you more.
We're also looking at ways to stop people having unnecessary operations by funding research into better ways to assess what’s causing their shoulder problems, based on their lifestyle and the way they do things.
The aim is to find the best treatment that is most likely to work for them. This could reduce the long-term pain, disability and time off work caused by their condition. Our information on developing a better approach to assess and treat shoulder pain will tell you more about this research.